Physiotherapy After Mastectomy
Introduction
Breast cancer is the leading cause of death and morbidity in women, and it’s the most prevalent malignancy. It is estimated that there are around 1.67 million breast cancer cases worldwide every year. There are also 458,000 annually related deaths. Breast cancer treatment is successful for 89%. However, some side effects of the surgery may last months to years. By calculating the prevalence of pain and joint dysfunction of upper limb as the most frequent side effect, we found that there was a difference between 12% and 51% (for pain) and 1.5% or 50% (for joint dysfunction). [ The study showed that shoulder pain is more common in patients suffering from mammary carcinoma who had lower values on the Karnofsky Perform Status scale and higher scores on the Social Communication Questionnaire. These risks are increased by poor socioeconomic standing, poor physical condition and non-Caucasian ethnicity, along with a patient’s score on the Quality of Lifescale. Research has shown that pain predictors include the severity of shoulder pain before surgery and the age of the patients. Moderate pain sufferers who underwent extensive axillary and mastectomy had a higher percentage. These patients have more lymph nodes removed and positive nodes. There are also more drainages that were placed during the surgery. In patients with moderate pain, there is an increased risk of complications.
The preoperative assessment and the educational booklet are combined in many cases. These include a summary, as well as the recommendations, for patients to follow up on their surgical procedure. McNeely’s study highlights the advantages of a supervised rehabilitation intervention over a standard one. The booklet contains an overview, educational materials, as well as unstructured and non-individualized exercises. Due to prompt detection of symptoms, personalized physical therapy has shown the potential to lower complex postoperative complications related to mammary tumors. It is, therefore, essential to recognize the most effective treatment based on the pain presented by the patient. Because breast cancer treatment directly involves the neuromusculoskeletal tissues in one or several limbs, it can cause shoulder pain, joint restriction, hyposthenia, or musculoskeletal discomfort. Shoulder pain due to mammary carcinoma treatment can actually be broken down into various types of pain. Patients with breast cancer may have a decreased range of motor strategies, resulting in movements that are less precise and causing pain. In Ebaugh’s study, it is stated that postural pain, scar formation, and protection posture cause a shortening of the small pectoral and large pectoral muscles [ ]. The posture can be characterized as a depression and an antepositioning. This misalignment can be exacerbated by radiation therapy or subsequent tissue fibrisis. It would cause an inexact relationship between the scapula, the chest wall, and between the head of the glenoid fossa. These structural changes can become chronic in the musculoskeletal tissues related to the shoulder, eventually causing pain.
You can divide neuropathic and drug-induced pain into three categories: neuropathy due to cancer; neuropathy caused by drugs, and neuropathy associated with the treatment of cancer. Postmastectomy pain syndrome is a common example of neuropathic pain induced by cancer therapy. Radiation therapy can cause neuropathy. It can even affect surrounding structures like the nerves, neural plexus, and nerves. Finally, neuropathic pain can be drug-induced by taking aromatase inhibitor drugs. They are the most frequently used hormonal treatment for the treatment of hormone-responsive tumors, which boasts the greatest scientific evidence [ However, about 50% of patients taking anti-aromatases report widespread musculoskeletal pain, defined as “aromatase inhibitor musculoskeletal syndrome,” which persists even after stopping the drug. This is manifested as arthralgia and osteoporosis. The onset of arthromial pain is reported as the most frequent cause of treatment suspension [ ]. Lipps analyzes data on radiotherapy side effects. Radiation therapy is an effective treatment to treat mammary carcinoma. However, there are some cases where patients experience side effects in the ipsilateral arm. Pain, skin reactions, and fatigue are some of the most commonly reported side effects. More than 60% of patients feel pain following treatment, while 4% report severe or very serious pain. Radiation therapy of muscles and connective tissues within the shoulder joint can lead to the formation of fibrosis and atrophy and, therefore, to pain.
Finally, chronic pain occurs in a proportion of up to 50% of patients six months after surgery [ ]. Chronic breast cancer survivors have higher rates of depression and more anxiety than women without a history of breast cancer. A significant risk factor for chronic pain syndrome is poorly managed postoperatively. It is believed that 25% to 60% of survivors of breast cancer experience persistent, unresolved pain after surgery. This can lead to motor dysfunction and a reduced quality of living. Certain patients who experience chronic pain are susceptible to central pain sensorization. This means that there is an increased risk of developing pain syndromes at the level below the brain.
Review
Methods Research Question: What physiotherapy treatments are most effective in treating shoulder pain for women with mammary cancer?
Eligibility Criteria *P – Patients who are being treated for mammary tumours with shoulder pain. The treatment options include surgery such as mastectomy and axillary node dissection. Sentinel lymph node biopsy is also available. Anti-aromatase medications and radiotherapy are some of the other treatments. *I (intervention): Physiotherapeutic interventions recognized by scientific evidence useful for the reduction of pain presented by patients following treatments for mammary carcinoma. Patients who only receive standard/usual assistance. In many studies, it is represented by preoperative counseling followed by the delivery of informative booklets. *O (results), a definition of rehabilitation intervention that demonstrates efficacy. It is based upon the diagnosis of shoulder pain in patients who have received treatment for mammary cancer.
Due to all studies being in English, the linguistic limitation was chosen. Additionally, the temporal restriction for studies is from the last ten years (2009-2019), when it was possible read only the abstract followed by the whole text.
All articles selected were correlated with shoulder pain due to mammary carcinoma, and the physiotherapy that was used to treat it.
Sources of Information and Research. The PubMed and Medline databases, CINAHL and Cochrane databases were utilized to find relevant publications for the 15-year period 2004-2019. The research used the following Boolean operators to locate PubMed, Medline, CINAHL and CINAHL publications:
((((“Upperextremity “[Mesh] AND upper Extremit* + pain OR Upper Limb* * AND pain*), AND (((“Breast Newplasms”[Mesh] AND (“Shoulder”[Mesh] AND shoulder *))), and (“Physical Therapy Modalities”, [Mesh] AND Physical Therapy Modalit* OT Physical Therapy Techniqu* OP Physiotherap* TECHN* Mechalit* TY Tecnalit* Physiotherap* &# OR physiotherapy Techn* PLAlit* TUQU* TY TECHN* Physiotherap* QUI*)
breast cancer or breast neoplasm or breast carcinoma or breast tumor and physiotherapy or physical therapy or physiotherapist or physical therapist and shoulder pain Study Selection The total number of articles identified through mesh research is 682 studies. Two-hundred ninety-nine articles were excluded because they did not meet the inclusion criteria, 258 articles were excluded after reading the abstract, and a further 112 after reading the full article text. The research question was relevant and useful in 13 of the thirteen articles, which included four systematic review, three narrative, and two randomized controlled trials. One uncontrolled trial and two pilot studies were also excluded (Table ).

Abstract
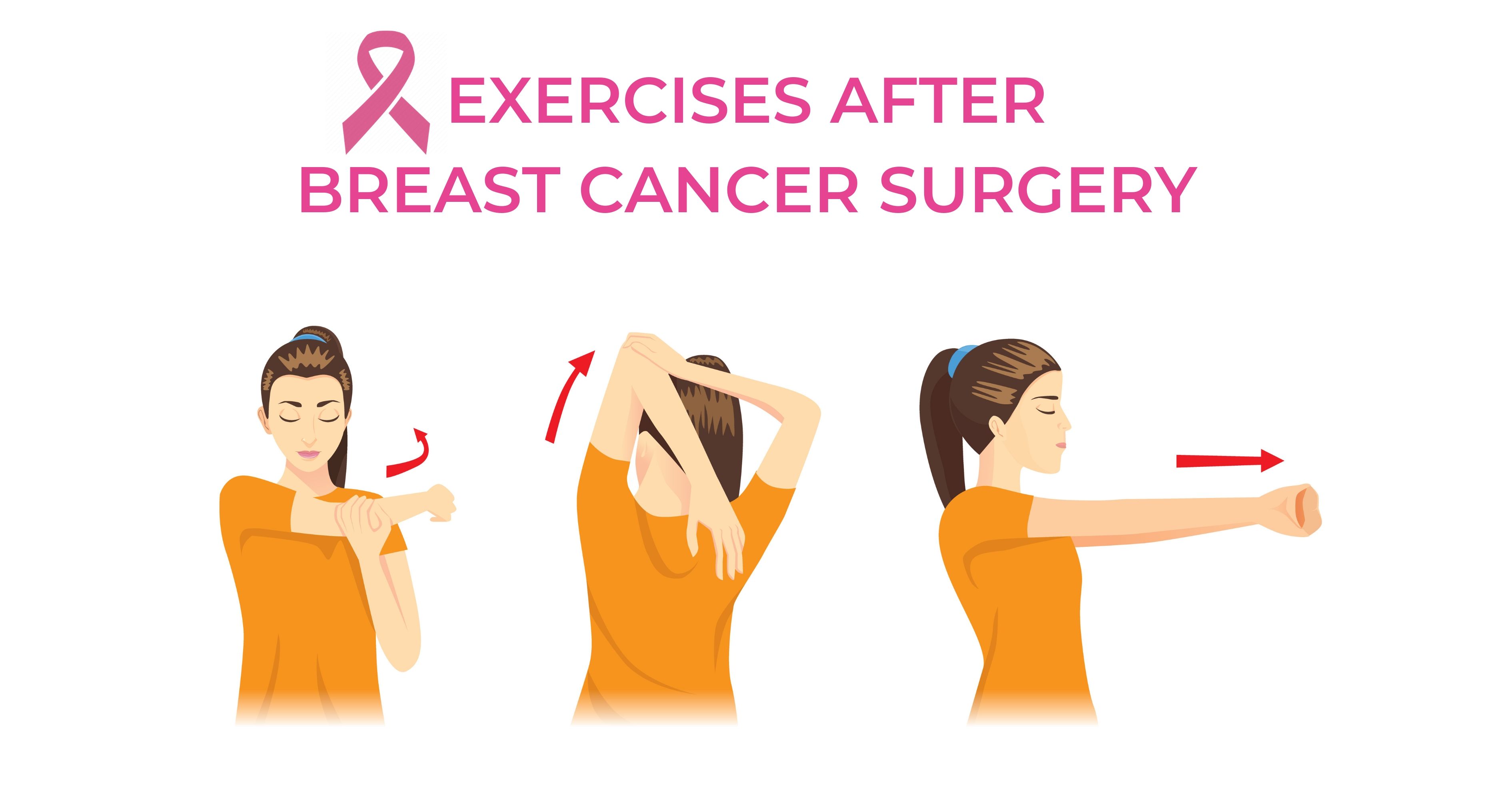
Background: Seromas and impaired shoulder function can be complications of modified radical mastectomy. For shoulder dysfunction prevention, early postoperative physical therapy is recommended. It was determined that delayed shoulder exercises, which are not associated with shoulder dysfunction, could decrease the number of postoperative seromas.
Methods Patients were seen by the surgeons and the physiotherapists during hospital stay and in the outpatient department. Surgery registered all serious conditions and any other problems. The physiotherapists advised the patients before and after surgery and measured shoulder function.
Results: Patients who underwent physiotherapy immediately after their operation (38%) had a higher rate of seromas than patients who were treated post-operatively (72%). (p 0.0.05). No significant differences were observed in shoulder function after surgery.
Delaying shoulder exercises for one week after a modified radical breastectomy is able to reduce the incidence of seromas. Postoperative physiotherapy should not be performed earlier to prevent impaired shoulder function.
.Physiotherapy After Mastectomy
Kent Chiro-Med Wellness Clinic
| Website | https://www.kentchiromed.com/ |
| Address | 563 Gladstone Ave, Ottawa, ON K1R 5P2, Canada |
| Phone | +1 613-508-0113 |
| Category | Physiotherapy Ottawa |
Beverly Physiotherapy
| Website | http://www.beverlyphysiotherapy.com/ |
| Address | 747 Ellice Ave, Winnipeg, MB R3G 0B5, Canada |
| Phone | +1 204-774-8385 |
| Category | Physiotherapy Winnipeg |















:fill(white "Amazon Cancellation Policy 2022")