Vibration Chest Physiotherapy

Similar Articles
[Physiotherapy in chronic obstructive pulmonary disease: oscillatory breathing with flutter VRP1].
Weiner P, Zamir D, Waizman J, Weiner M. Weiner P, et al. Harefuah. 1996 Jul;131(1-2):14-7, 71. Harefuah. 1996. Clinical Trial. Hebrew.
Chest physiotherapy to treat chronically ill patients.
Bateman JR, Newman SP, Daunt KM, Pavia D, Clarke SW. Bateman JR, et al. Lancet. 1979 Feb 10;1(8111):294-7. doi: 10.1016/s0140-6736(79)90705-0. Lancet. 1979. Clinical Trial.
The pulmonary hemodynamics of patients with chronic, obstructive pneumonia disease can be improved by in-phase chest wall vibration.
Nakayama H, Shibuya M, Kaneko N, Yamada M, Suzuki H, Arakawa M, Homma I. Nakayama H, et al. Respirology. 1998 Dec;3(4):235-40. doi: 10.1111/j.1440-1843.1998.tb00128.x. Respirology. 1998. PMID: 10201049 Chest physiotherapy: a review.
Sutton PP, Pavia D, Bateman JR, Clarke SW. Sutton PP, et al. Eur J Respir Dis. 1982 May;63(3):188-201. Eur J Respir Dis. 1982. PMID: 7047185 Review.
Paediatrics aged 0-24 months receive chest physiotherapy in acute bronchiolitis.
Perrotta C, Ortiz Z, Roque M. Perrotta C, et al. Cochrane Database Syst Rev. 2005 Apr 18;(2):CD004873. doi: 10.1002/14651858.CD004873.pub2. Cochrane Database Syst Rev. 2005. PMID: 15846736 Updated. Review.
Abstract
Objective: To investigate the effects of chest wall vibration timing on air flow and pressure in a ventilated lung model.
Design: An experimental bench study.
Participants: Thirty experienced physiotherapists in intensive care.
Intervention: The physiotherapists used eight sets chest wall vibrations on an intubated, mechanically ventilated model. The vibrations were used at three points: the beginning of expiration (optimal), during mid-to late inspiration (early), and in the early stages of expiration or mid-to mid expiration. The continuous measurement of volume, peak pressure, air flow and volume was done. The force applied to vibrations was recorded with a force sensor mat placed underneath the hands of physiotherapists.
The results showed that peak expiratory flow was significantly higher during optimal and early vibrations than baseline ventilation. Inexpiratory flow was not enhanced by late vibrations. Inflection pressure reached its peak during early vibrations, which was significantly more than the baseline value (mean difference between baseline and early vibrations: 5.6cmH(2)O at 95% CI 2.9 to 8.2). Average peak inspiratory power during the early vibrations averaged 8.4 cmH(2)O less than for optimal timing.
Final conclusion: Timing of vibrations during the breath cycle is likely to influence the effectiveness and safety of respiratory therapy treatments. High peak inspiratory pressures could be deadly if early vibrations occur. While not necessarily harmful, late vibrations do not increase peak expiratory flow. This is an important consideration when training physiotherapists and evaluating outcomes of treatments in intensive care.
Copyright (c), 2010 Chartered Society of Physiotherapy. Published by Elsevier Ltd. All Rights Reserved.

Similar Articles
A study that found manual vibration to increase the expiratory flow rate in healthy adults through an increased intrapleural tension.
McCarren B, Alison JA, Herbert RD. McCarren B, et al. Aust J Physiother. 2006;52(4):267-71. doi: 10.1016/s0004-9514(06)70006-x. Aust J Physiother. 2006. PMID: 17132121 Clinical Research
Physiological effects of vibration in subjects with cystic fibrosis.
McCarren B, Alison JA. McCarren B, et al. Eur Respir J. 2006 Jun;27(6):1204-9. doi: 10.1183/09031936.06.00083605. Epub 2006 Feb 2. Eur Respir J. 2006. PMID: 16455834 Clinical Trial.
The unique contribution of manual chest compression-vibrations to airflow during physiotherapy in sedated, fully ventilated children.
Gregson RK, Shannon H, Stocks J, Cole TJ, Peters MJ, Main E. Gregson RK, et al. Pediatr Crit Care Med. 2012 Mar;13(2):e97-e102. doi: 10.1097/PCC.0b013e3182230f5a. Pediatr Crit Care Med. 2012. PMID: 266530 Clearance of high-frequency airways by assisted technology
Chatburn RL. Chatburn. Respir Care. 2007 Sep;52(9);1224-35. Discussion 1235-7. Respir Care. 2007. PMID: 17716388 Review.
Airway clearance therapy in cystic fibrosis patients.
Pisi G, Chetta A. Pisi G, et al. Acta Biomed. 2009 Aug;80(2):102-6. Acta Biomed. 2009. PMID: 19848046 Review.
Chest Physiotherapy
Andrea R. Levine Jason Stankiewicz. For patient education, click here. Chest therapy uses external mechanical maneuvers like chest percussion and postural drainage to increase the mobilization of and clear airway secretions. This is for those patients whose cough cannot clear its thick, persistent, copious or located secretions. (General references) Chest physiotherapy uses external mechanical maneuvers such as vibration, postural drainage and chest percussion to increase mobilization. It’s indicated… continue reading Bronchiectasis Bronchiectasis Bronchiectasis causes dilation and disintegration of the larger bronchi due to chronic inflammation and infection. Cystic Fibrosis, immuno defects and recurrent infection are common causes. Chronic Obstructive Pulmonary disease (COPD), also known as Chronic Obstructive Pulmonary Disorder (COPD), is an inflammation response that results in airflow restriction. This can often be caused by inhaled toxic substances, such as cigarette smoke. Alpha-1 antitrypsin deficiency and various occupational… read more (chronic obstructive pulmonary disease), in certain clinical situations ( General references Chest physiotherapy consists of external mechanical maneuvers, such as chest percussion, postural drainage, and vibration, to augment mobilization and clearance of airway secretions. It is indicated… read more Cystic fibrosis Cystic Fibrosis Cystic fibrosis is an inherited disease of the exocrine glands affecting primarily the gastrointestinal and respiratory systems. Pneumonia, which is an inflammation of the lung caused by infection, can be a chronic condition that leads to exocrine insufficiency and ex-lung disease. The chest xray is the most important factor in diagnosing pneumonia. There are many factors that can cause, treat, or prevent cystic fibrisis. You can develop chronic lung disease or exocrine-pancreatic insufficiency. Read more

Chest Physiotherapy during Mechanical Ventilation
Some patients can lose their spontaneous breathing due to mechanical ventilation. This can predispose the patients to developing lung collapse and ventilator-associated pneumonia. In such circumstances, chest physiotherapy can be used to reduce the length of stay in both a mechanical ventilator and ICU and prevent ventilator-associated pneumonia ( ). In addition, high-frequency chest wall oscillation for intubated patients resulted in increased dry sputum weight and PaO on day 3, decreased lung collapse on days 2 and 3, and culture positivity on day 3 ( ). In a similar vein, a patient who had received eleven sessions physical therapy (comprising upright body positioning, mobilization, exercise, and an active cycle to breathing exercise technique) over a 48-hour ICU stay (six sessions per day on day one, five sessions each day on day two), his arterial oxygen level significantly improved, as well as radiographic resolution of any infiltration. Therefore, since chest physiotherapy reverses pathological progression, prevents atelectasis, improves impaired gas exchange, and decreases culture positivity, which are also some of the pathological hallmarks of COVID-19, it can be utilized in patients with this disease.
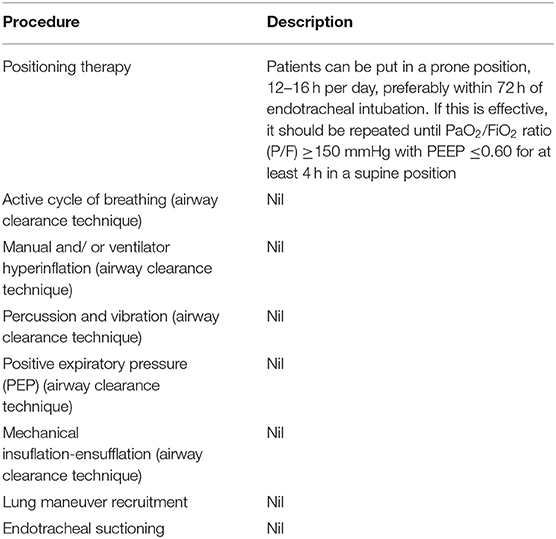
Patients who use a ventilator should be aware of the following: airway clearing techniques, lung maneuver recruitment and endotracheal succioning. The airway clearance techniques recommended include positioning, active cycle of breathing, manual and/or ventilator hyperinflation, percussion and vibration, positive expiratory pressure (PEP), and mechanical insuflation-ensufflation ( ). There aren’t any details about how these techniques should be performed, except for positioning therapy. Also, no reports have yet been done on COVID-19 patients regarding the effectiveness of these techniques. Details of positioning therapy can be found in Table 1. Additionally, you should exercise extreme caution with lung maneuver recruitment. Chest physiotherapy is not recommended during this time. This depends on how the patient’s neurological, respiratory and cardiovascular functions are. For more information on the contraindications, see Table 2.
Physiotherapeutic Intervention
Chest physiotherapy was administered to the subjects in this study. The treatment took approximately fifteen minutes. After being diagnosed with septic shock, the subjects in this study were treated for their first chest therapy. The chest maneuvers were performed by all the subjects when they were placed dorsally in decubitus. To increase or redirect the air flow for pulmonary improvement and clearance and to prevent pulmonary collapse, expiratory compression of the rib cage involves pressing mechanical forces through the chest wall.
These vibrations were made by isometric contractions and synchronization of the palms perpendicularly to the chest.
Manual hyperinflation was accomplished using an Ambu, Glen Burnie and Maryland manual hyperinflation apparatus. Inflation pressure was 40 cm HO and F at 0,6. This inducing an increase in tidal volume, inspiratory circulation, and then bronchial secretion clearance.
As part of the tracheal aspiration process, manual hyperinflation took place simultaneously. There were 5-6 ventilatory rounds at each tracheal aspiration. For tracheal extraction, we used a size 10 or12 aspiration catheter (CPL Medicals Sao Paulo Brazil), and saline solution 0.9% (using a maximum of 10 mL for the entire aspiration process). This was applied slowly to reduce secretions.
According to the amount of secretions, how many aspirations were performed was a factor in determining the number. Vacuum level was set at 30 cm Hg.
S, Heart Rate, Breathing Frequency, and Mean Arterial Pressure were all monitored during the implementation of these techniques to monitor the effects (data not displayed).
How is Vibration in Chest Physiotherapy Different?
A manual technique that respiratory physiotherapists use to remove phlegm (secretions) from the chest is called vibrations.
How is Vibration in Physiotherapy Different?
Vibration therapy uses vibration as a physical tool during treatment. Vibration refers to the propagation elastic waves that produce deformations or tensions in a continuously moving medium. The vibratory movement is very short and fast and repeated around an equilibrium position.2 Nov 2021
Which are the 3 techniques used in chest physiotherapy treatment?
Chest physical therapy (CPT or Chest PT) is an airway clearance technique (ACT) to drain the lungs, and may include percussion (clapping), vibration, deep breathing, and huffing or coughing.
How can I get my stomach to vibrate?
Step 4 Next, breathe out the person and then vibrate the affected area with your hands. After vibrating the chest at least three times, assist the patient with coughing. When vibrating, it is important to keep the muscles of the arms and hands tense. Use pressure to vibrate your hands and arms.
.Vibration Chest Physiotherapy
Kent Chiro-Med Wellness Clinic
| Website | https://www.kentchiromed.com/ |
| Address | 563 Gladstone Ave, Ottawa, ON K1R 5P2, Canada |
| Phone | +1 613-508-0113 |
| Category | Physiotherapy Ottawa |
Beverly Physiotherapy
| Website | http://www.beverlyphysiotherapy.com/ |
| Address | 747 Ellice Ave, Winnipeg, MB R3G 0B5, Canada |
| Phone | +1 204-774-8385 |
| Category | Physiotherapy Winnipeg |
















:fill(white "Amazon Cancellation Policy 2022")
